Annals of Middle Eastern Medicine
Maysoon Aladham et al. Annals of Middle Eastern Medicine. 2026;2(1):015-021
ORIGINAL ARTICLE
Association between estimated blood loss and hemoglobin decline in instrumental vaginal delivery: a retrospective cross-sectional study in Riyadh, Saudi Arabia
Maysoon Aladham1*, Rana Ayed Alayed2, Ghaida Mubarak Alotaibi2, Deema Sameer Alzahrani2, Fardus Salem Alsaiary2, Hafiza Turkistany1
Correspondence to: Maysoon Aladham
*OBGYN Department, Women’s Health Hospital, NGHA, Riyadh.
Email: Adhamm@mngha.med.sa
Full list of author information is available at the end of the article.
Received: 07 March 2026 | Revised (1): 14 March 2026 | Revised (2): 18 March 2026 | Accepted: 25 March 2026
ABSTRACT
Background:
Instrumental vaginal delivery (IVD) is an essential component of obstetric care aimed at facilitating vaginal delivery and reducing maternal and neonatal morbidity and mortality. However, it may be associated with postpartum hemoglobin decline due to blood loss.
Objectives:
To evaluate postpartum hemoglobin drop following IVD and determine whether Estimated blood loss (EBL) independently predicts clinically significant hemoglobin decline.
Design:
Retrospective cross-sectional study.
Settings:
National Guard Hospital, Riyadh, Saudi Arabia.
Patients and Methods:
This study included 320 women who underwent IVD between September 2023 and October 2024. Data were collected from electronic medical records, including demographic characteristics, type of instrumental delivery, pre- and post-delivery hemoglobin levels, and EBL. Statistical analysis was performed using SPSS software.
Main Outcome Measures:
Continuous hemoglobin drop and ≥2 g/dL decline.
Sample Size:
Of 320 eligible patients, 297 with complete hematologic data were analyzed.
Results:
Mean pre-delivery hemoglobin declined significantly postpartum (P < 0.001), and 19.9% experienced ≥2 g/dL reduction. EBL independently predicted hemoglobin decline (0.30 g/dL decrease per 100 mL; P < .001). Each 100 mL increase in EBL increased the odds of a significant decline by 55% (OR 1.55; P < 0.001). ROC analysis showed acceptable discrimination (AUC 0.75). An EBL threshold of 400 mL yielded 80% sensitivity, 64% specificity, and 93% negative predictive value.
Conclusion:
EBL independently predicts postpartum hemoglobin decline after IVD. A 400 mL threshold may help identify patients at risk for clinically significant reduction and guide selective early hemoglobin assessment.
Strengths:
Targeted focus on instrumental deliveries, multivariable-adjusted analysis, and identification of a clinically actionable blood loss threshold.
Limitations:
Retrospective design and reliance on visually estimated blood loss.
Keywords:
Hemoglobin, Instumental vaginal delivery, estimated blood loss.
Introduction
Postpartum anemia remains a common complication of childbirth and represents an important contributor to maternal morbidity worldwide. Hemoglobin is the primary oxygen-carrying protein in red blood cells and plays a critical role in transporting oxygen from the lungs to peripheral tissues while facilitating the return of carbon dioxide to the lungs [1,2]. In obstetric practice, decreases in hemoglobin concentration commonly reflect intrapartum blood loss combined with physiological fluid shifts. Although modest reductions in hemoglobin levels are expected following delivery, substantial declines may delay maternal recovery, contribute to fatigue, and increase the risk of postpartum anemia requiring medical intervention [3]. Postpartum hemorrhage (PPH) remains one of the leading causes of maternal morbidity and mortality globally. According to the World Health Organization, PPH is defined as cumulative blood loss of ≥1000 mL within 24 hours after birth or blood loss associated with signs or symptoms of hypovolemia [4,5]. Recent global estimates indicate that PPH accounts for approximately 20%-30% of maternal deaths worldwide, making it a major public health concern, particularly in low- and middle-income countries [5,6]. The severity of PPH may be influenced by several factors, including uterine atony, genital tract trauma, retained placental tissue, coagulation disorders, and mode of delivery [7,8]. Severe hemorrhage may result in significant maternal complications such as hypovolemic shock, organ dysfunction, prolonged hospitalization, and increased risk of postpartum anemia [8].
Instrumental vaginal delivery (IVD), which includes vacuum-assisted and forceps-assisted delivery, plays an important role in modern obstetric practice by facilitating vaginal birth when complications arise during the second stage of labor [9,10]. IVDs may be performed to shorten the second stage of labor in the presence of maternal exhaustion, non-reassuring fetal heart rate patterns, or when maternal medical conditions necessitate expedited delivery. Compared with spontaneous vaginal delivery, IVDs may be associated with increased genital tract trauma and greater intrapartum blood loss. In contrast to cesarean delivery, however, IVDs may reduce surgical complications and recovery time [10]. In Saudi Arabia, several studies have evaluated the prevalence of IVDs. One regional study conducted in Qassim, Saudi Arabia, reported that only 2.2% of 936 women underwent IVD, compared with higher proportions of spontaneous vaginal delivery and cesarean section [11].
Accurate estimation of blood loss during childbirth is essential for early detection of postpartum hemorrhage and prevention of maternal complications. However, in routine clinical practice, blood loss during delivery is most commonly documented using visual estimation by the attending healthcare team. Several studies have demonstrated that visually estimated blood loss (EBL) frequently underestimates the actual volume of hemorrhage and is associated with considerable interobserver variability [12,13]. This limitation may delay recognition of clinically significant blood loss and subsequent hemoglobin decline, particularly in cases where postpartum laboratory evaluation is not routinely performed.
Despite the clinical importance of postpartum blood loss assessment, limited studies have evaluated the quantitative relationship between EBL and objectively measured postpartum hemoglobin decline following IVD. Furthermore, clinically meaningful blood loss thresholds that may predict significant hemoglobin reduction have not been clearly established in real-world obstetric practice.
Therefore, the aim of this study was to evaluate postpartum hemoglobin decline following IVD and to determine whether EBL independently predicts clinically significant hemoglobin reduction in a tertiary-care hospital in Riyadh, Saudi Arabia.
Methods
Study design and setting
This retrospective cross-sectional study was conducted at the Women’s Health Hospital, National Guard Hospital, Riyadh, Saudi Arabia, a tertiary-care center providing comprehensive obstetric services, including high- and low-risk deliveries. The study evaluated postpartum hemoglobin decline following IVD and examined its relationship with EBL within routine clinical practice.
Inclusion and exclusion criteria
The inclusion criteria for eligibility were as follows: (a) women aged 18-60 years, (b) women who underwent IVD, and (c) deliveries occurring between September 2023 and October 2024. The exclusion criteria included: (a) women who delivered via spontaneous vaginal delivery or cesarean section to ensure a homogeneous cohort of instrumental deliveries, and (b) cases with incomplete hemoglobin data, specifically those missing either pre-delivery or post-delivery hemoglobin values.
Sample Size Calculation
Sample size was calculated using the Raosoft sample size calculator with a 95% confidence level, 5% margin of error, and assumed response distribution of 50%, yielding a minimum required sample of 197 participants. A total of 320 eligible patients met the inclusion criteria. Cases with incomplete hemoglobin data (either missing pre- or post-delivery hemoglobin values) were excluded from multivariable analyses.
Data collection and variables
Data were extracted from the BestCare electronic medical record system (BestCare EMR, Version 8, ezCaretech Co., Seoul, South Korea). Collected variables included maternal age, body mass index (BMI), parity, type of instrumental delivery (Kiwi vacuum, metallic vacuum, or forceps), EBL (mL), pre-delivery hemoglobin, post-delivery hemoglobin, and presence of chronic disease.
EBL was documented by the attending clinical team using routine visual estimation methods in accordance with institutional practice. The primary outcome variable was postpartum hemoglobin drop, calculated as: Hb drop = Pre-delivery Hb − Post-delivery Hb. This approach has been commonly used in clinical studies evaluating blood loss–related hemoglobin decline [14]. Postpartum hemoglobin was obtained as part of routine clinical care; exact timing varied and was not standardized. To enhance clinical applicability, a secondary outcome variable was defined as clinically significant hemoglobin decline, defined a priori as ≥2 g/dL reduction from baseline, which has been used in previous clinical investigations evaluating postpartum anemia and blood loss [15]. Independent variables included EBL (continuous), baseline hemoglobin, maternal age, BMI, parity, instrument type, and chronic disease status.
Statistical analysis
Data were exported to Microsoft Excel for verification and subsequently analyzed using SPSS version 24 (IBM Corp., Armonk, NY). Continuous variables were summarized as mean (standard deviation) or median (interquartile range) based on distribution normality assessed using the Shapiro–Wilk test [16]. Categorical variables were presented as frequencies and percentages. Univariate analyses were initially performed to explore associations between EBL and hemoglobin decline.
To address potential confounding, multivariable linear regression analysis was conducted with continuous hemoglobin drop as the dependent variable. Independent variables entered into the regression model included EBL, baseline hemoglobin, maternal age, BMI, parity, instrument type, and chronic disease status. Multivariable logistic regression analysis was additionally performed to identify predictors of clinically significant hemoglobin decline (≥2 g/dL). Adjusted odds ratios (OR) and 95% confidence intervals (CI) were reported.
To evaluate the predictive performance of EBL, receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive performance of EBL. ROC analysis is widely used to assess the diagnostic accuracy of continuous predictors [17]. The area under the curve (AUC) was calculated to assess discriminatory ability, and the optimal cutoff value was identified using the Youden index. Sensitivity, specificity, positive predictive value, and negative predictive value (NPV) were calculated. Model assumptions for regression analyses were assessed, and multicollinearity was evaluated using variance inflation factors. Statistical significance was defined as P < 0.05 (two-tailed).
Ethical considerations
This study was approved by the King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia (approval no. NRR24/036/8). Patient confidentiality was strictly maintained, and all data were anonymized prior to analysis. The study was conducted in accordance with institutional ethical guidelines and the Declaration of Helsinki.
Results
A total of 320 women underwent IVD during the study period. After exclusion of cases with incomplete hemoglobin data, 297 women were included in the multivariable analysis, Table 1. The study population was characterized by a high prevalence of elevated body mass index, with a significant proportion of participants being classified as either overweight or obese, Table 1.
Table 1. Demographic and clinical characteristics of the study population.
| Characteristic | N = 320a |
|---|---|
| Age | 29.0 (26.0, 32.0) |
| Weight | 69 (63, 80) |
| Height | 157.0 (153.5, 160.0) |
| BMI | 28.2 (25.0, 31.9) |
| Body mass index | |
| Underweight | 4 (1.3%) |
| Healthy weight | 74 (23%) |
| Overweight | 121 (38%) |
| Obese | 121 (38%) |
| Chronic diseaseb | |
| DM | 36 (40%) |
| GDM | 31 (34%) |
| Hypothyroidism | 26 (29%) |
| BA | 5 (5.6%) |
| Hematological disease | 5 (5.6%) |
| HTN | 4 (4.4%) |
| Heart disease | 3 (3.3%) |
| GHTN | 2 (2.2%) |
| Others | 9 (10%) |
| Missing | 230 |
a) Median (IQR); n (%)
b) Multi-choice question
Regarding obstetric outcomes, the majority of women were nulliparous (55%) and primarily underwent vacuum-assisted delivery, with the Kiwi method being the most frequently utilized instrument (61%), Table 2. The median EBL recorded for these deliveries was 300 mL (IQR 200-400), Table 2.
There was a statistically significant reduction in mean hemoglobin levels from the pre-delivery to the postpartum period (P < 0.001), a trend clearly visualized in the downward shift shown in Figure 1. Clinically meaningful hemoglobin depletion, defined as a drop of ≥2 g/dL, affected approximately one-fifth of the women in this cohort.
Factors associated with postpartum hemoglobin drop
The association between maternal characteristics, perinatal factors, and post-delivery hemoglobin levels is presented in Table 3. On univariate analysis, increasing EBL demonstrated a graded relationship with greater hemoglobin decline, where women with higher blood loss categories experienced progressively larger reductions in hemoglobin. However, because hemoglobin decline may be influenced by multiple maternal and obstetric variables, multivariable regression models were used to isolate the primary drivers of this drop.
In multivariable linear regression analysis, EBL remained a strong independent predictor of postpartum hemoglobin decline, Table 3. Specifically, incremental increases in blood loss were directly proportional to the magnitude of the hemoglobin drop (P < 0.001), whereas the specific type of instrument used did not remain a significant factor after adjusting for blood loss and maternal characteristics.
Table 2. Mode of delivery and maternal outcomes of pregnant women.
| Characteristic | N = 320 |
|---|---|
| Forcepsa | |
| No | 296 (93%) |
| Yes | 24 (7.5%) |
| Metallica | |
| No | 218 (68%) |
| Yes | 102 (32%) |
| Vacuum-assisted delivery (KIWI)a | |
| No | 126 (39%) |
| Yes | 194 (61%) |
| Hemoglobin level pre-deliveryc | 118.9 (11.3) |
| Missing | 4 |
| Hemoglobin level post-deliveryc | 111.8 (11.8) |
| Missing | 7 |
| Estimated blood loss in millilitersb | 300 (300, 400) |
| Missing | 2 |
| Number of previous deliveriesa | |
| 0 | 169 (55%) |
| 1-3 | 89 (38.8%) |
| 4-6 | 16 (5%) |
| Missing | 11 |
a) n (%)
b) Median (IQR)
c) Mean (SD)
Predictive performance of EBL
In multivariable logistic regression analysis, EBL was the strongest independent predictor of significant hemoglobin decline. Each 100 mL increase in blood loss was associated with a 55% increase in the odds of experiencing a ≥2 g/dL drop (OR 1.55; P < 0.001). ROC analysis demonstrated acceptable discriminatory ability of EBL for predicting this decline (AUC = 0.75). An identified optimal cutoff of 400 mL demonstrated a high NPV, suggesting that documented blood loss below this threshold serves as a reliable indicator that a clinically meaningful hemoglobin reduction is unlikely.
Discussion
This study evaluated postpartum hemoglobin decline following IVD and examined the relationship between estimated blood loss and clinically significant hemoglobin reduction. The results demonstrated a significant decrease in hemoglobin levels after delivery, with approximately one-fifth of women experiencing a decline of ≥2 g/dL. Importantly, EBL remained an independent predictor of hemoglobin decline after adjustment for maternal and obstetric factors. Furthermore, ROC analysis identified an estimated blood loss threshold of approximately 400 mL that was associated with increased likelihood of clinically meaningful hemoglobin reduction.
The findings of this study regarding the correlation between hemoglobin drop and postpartum blood loss are consistent with those reported by Mansukhani et al., who concluded that increased postpartum hemorrhage contributes to lower post-delivery hemoglobin levels. Specifically, they demonstrated that a decrease in hemoglobin levels prior to delivery was associated with increased maternal adverse outcomes [18]. Similarly, Mohammed et al. reported that blood loss is a major contributing factor to postpartum anemia, with the risk increasing fivefold as blood loss increases. Furthermore, they demonstrated that parity had no significant association with the decline in hemoglobin levels, which is consistent with the findings of the present study regarding the effect of the number of previous deliveries on hemoglobin levels [19]. In the current study, a significant association was also observed between maternal age and post-delivery hemoglobin decline, where younger patients exhibited lower hemoglobin concentrations compared with older patients. This finding is supported by Rathod et al., who identified younger maternal age as a risk factor for the development of postpartum anemia [20]. Similarly, Atuahene et al. reported comparable findings, demonstrating an association between younger maternal age and hemoglobin decline following delivery [21]. Although hemoglobin levels were numerically lower in forceps-assisted deliveries and higher in vacuum-assisted deliveries (KIWI), this difference did not reach statistical significance in our study. In contrast, Abneh et al. reported that women who delivered via vacuum or forceps-assisted delivery had a threefold increased risk of developing postpartum anemia [22].
The findings of this study are consistent with previous reports demonstrating increased postpartum anemia in the setting of greater blood loss [19,20,22]. However, prior studies have largely reported unadjusted associations or focused on postpartum hemorrhage categorization rather than continuous hemoglobin decline. By incorporating multivariable modeling and predictive analysis, this study contributes additional granularity and clinical applicability to existing literature.
Interestingly, instrument type did not independently predict hemoglobin reduction after multivariable adjustment. Although forceps-assisted deliveries demonstrated numerically lower post-delivery hemoglobin levels, these differences were not statistically significant. This suggests that the magnitude of blood loss, rather than instrument type, may be the more relevant determinant of postpartum hematologic change within instrumental deliveries. Our ROC analysis demonstrated acceptable discriminatory performance (AUC 0.75) of EBL for identifying patients at risk of significant hemoglobin decline. The high NPV (93%) at the 400 mL threshold suggests that patients with lower documented blood loss are unlikely to experience clinically significant hemoglobin reduction. This finding has direct clinical implications and may support selective rather than universal early postpartum hemoglobin testing in stable instrumental deliveries.
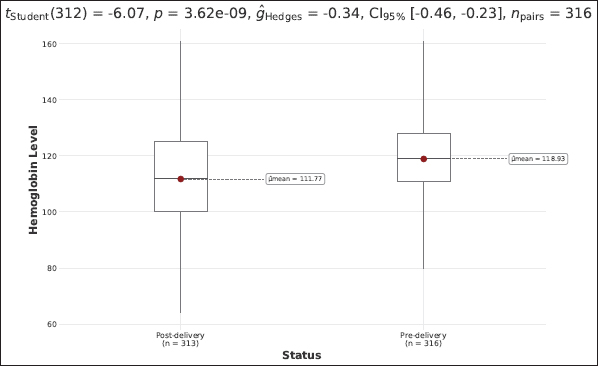
Figure 1. Association between pre-delivery and post-delivery hemoglobin levels.
Table 3. Maternal characteristics according to post-delivery hemoglobin decline.
| Characteristic | N = 320a | P-valueb |
|---|---|---|
| Age | 0.025 | |
| 17-29 | 110 ± 19 | |
| 30-47 | 114 ± 16 | |
| Body mass index | 0.20 | |
| Underweight | 123 ± 11 | |
| Healthy weight | 111 ± 18 | |
| Overweight | 110 ± 20 | |
| Obese | 114 ± 16 | |
| Number of previous deliveries | 0.12 | |
| 0 | 110 ± 19 | |
| 1 to 3 | 114 ± 16 | |
| 4 to 6 | 114 ± 15 | |
| Forceps | 0.50 | |
| No | 112 ± 18 | |
| Yes | 109 ± 20 | |
| Metallic | 0.20 | |
| No | 113 ± 18 | |
| Yes | 110 ± 18 | |
| KIWI | 0.11 | |
| No | 110 ± 18 | |
| Yes | 113 ± 18 | |
| Estimated blood loss | < 0.001 | |
| 100-300 | 117 ± 15 | |
| 301-600 | 109 ± 19 | |
| More than 601 | 94 ± 13 |
a) Hemoglobin level post-delivery: Mean ± SD
b) Welch two-sample t test; one-way ANOVA
While the relationship between EBL and hemoglobin decline is physiologically expected, our analysis quantifies this association and evaluates its predictive performance in a real-world clinical setting. The multivariable regression approach confirms that EBL remains an independent determinant of hemoglobin drop after accounting for baseline hemoglobin, BMI, parity, instrument type, and chronic disease status. This strengthens the validity of the association and addresses potential confounding factors that may influence measured hemoglobin decline. The observed decline in hemoglobin following increased blood loss is explained by both direct erythrocyte loss and subsequent hemodilution. Following acute hemorrhage, proportional plasma and red cell loss may initially mask laboratory changes. Subsequent redistribution of extracellular fluid and administration of intravenous fluids contribute to measurable reductions in hemoglobin concentration. These physiological processes likely account for variability in the magnitude of observed postpartum hemoglobin decline.
Several limitations warrant consideration. Visual estimation of blood loss is inherently subjective and may introduce measurement error. However, this reflects routine obstetric documentation practice and enhances the generalizability of findings to real-world settings. Additionally, variability in the timing of postpartum hemoglobin measurement and lack of standardized intrapartum fluid volume data may influence the degree of measured decline. Nevertheless, the consistent independent association between EBL and hemoglobin drop supports the robustness of the primary findings.
Overall, these results suggest that EBL during IVD is not merely descriptively associated with hemoglobin decline but provides quantifiable predictive value for clinically significant hematologic outcomes.
Strengths
This study has several strengths. First, it evaluates postpartum hemoglobin decline specifically in the context of IVD, an area that remains relatively under-studied in obstetric research. Second, the use of multivariable regression analysis allowed adjustment for multiple maternal and obstetric variables, strengthening the validity of the observed association between estimated blood loss and hemoglobin decline. Third, the study incorporated receiver operating characteristic analysis to identify a clinically meaningful blood loss threshold that may assist in postpartum risk stratification in routine clinical practice.
Limitations
This study has inherent limitations related to its retrospective cross-sectional design. Although multivariable regression modeling was employed to control for measured confounders, causal relationships cannot be definitively established, and the possibility of residual confounding cannot be entirely excluded. EBL was recorded using routine visual assessment, which may introduce measurement variability. However, this reflects standard obstetric documentation practice and enhances the real-world generalizability of the findings.
Variability in the timing of postpartum hemoglobin measurement and differences in fluid management practices may influence the magnitude of observed hemoglobin decline. Nevertheless, the consistent independent association observed across multivariable models suggests that the relationship between EBL and hemoglobin reduction remains robust. Finally, as a single-center study conducted in a tertiary-care hospital, findings should be interpreted in the context of institutional practice patterns. Future prospective studies incorporating quantitative blood loss measurement may further refine predictive performance.
Conclusion
EBL during IVD independently predicts postpartum hemoglobin decline after adjustment for maternal and obstetric factors. A blood loss threshold of approximately 400 mL demonstrated acceptable discriminatory performance for identifying patients at risk of clinically significant hemoglobin reduction (≥2 g/dL). These findings suggest that EBL may serve as a practical tool for postpartum risk stratification and support consideration of selective early hemoglobin assessment in higher-risk patients.
Acknowledgments
The authors acknowledge the contributions of the Research Department of KSAU, College of Medicine, and the OBGYN Department of NGHA throughout the process of this study.
Conflict of Interests
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding
No funding source
Consent for participation
This study was a cross-sectional study with data being extracted from Electronic medical records, therefore, patients’ consent was not necessitated. However, the privacy and confidentiality of all patients’ data were protected, as access to the data was limited to the investigator and co-investigators of this study.
Ethical Approval
Ethical approval was granted by Institutional Review Board (IRB) of KAIMRC, IRB Approval Protocol Number: NRR24/036/8, dated 08/14/2024.
Author details
Maysoon Aladham1, Rana Ayed Alayed2, Ghaida Mubarak Alotaibi2, Deema Sameer Alzahrani2, Fardus Salem Alsaiary2, Hafiza Turkistany1
- Department of Obstetrics and Gynecology, National Guard Hospital, Riyadh. Saudi Arabia
- College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh. Saudi Arabia
Supplementary content (If any) is available online.
References
- Billett HH. Hemoglobin and hematocrit. In: Walker HK, Hall WD, Hurst JW ed.s, Clinical Methods: the History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990.
- Marengo-Rowe AJ. Structure-function relations of human hemoglobins. Proc Bayl Univ Med Cent. 2006;19(3):239–45. https://doi.org/10.1080/08998280.2006.11928171
- Wang J, Wei J, Wang M. The risk factors of perioperative hemoglobin and hematocrit drop after intramedullary nailing treatment for intertrochanteric fracture patients. J Orthop Sci. 2015;20(1):163–7. https://doi.org/10.1007/s00776-014-0667-3
- Wormer KC, Jamil RT, Bryant SB. Postpartum hemorrhage. StatPearls [Internet]Treasure Island (FL): StatPearls Publishing; 2024. [cited 2026 Mar 17], Available from https://www.ncbi.nlm.nih.gov/books/NBK499988
- World Health Organization. WHO recommendations on the assessment of postpartum blood loss and use of a treatment bundle for postpartum haemorrhage. Geneva: World Health Organization; 2023.
- Say L, Chou D, Gemmill A, Tunçalp O, Moller AB, Daniels J, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–33. https://doi.org/10.1016/S2214-109X(14)70227-X
- Evensen A, Anderson JM, Fontaine P. Postpartum hemorrhage: prevention and treatment. Am Fam Physician. 2017;95(7):442–9.
- Oyelese Y, Scorza WE, Mastrolia R, Smulian JC. Postpartum hemorrhage. Obstet Gynecol Clin North Am. 2007;34(3):421–1. https://doi.org/10.1016/j.ogc.2007.06.007
- Cleveland Clinic. Types of delivery: childbirth options, differences & benefits [Internet]. Cleveland (OH): Cleveland Clinic; 2022. Available from: https://my.clevelandclinic.org/health/articles/9675-pregnancy-types-of-delivery. Accessed 17 Mar 2026.
- Garba J, Burodo A, Saidu A, Sulaiman B, Umar A, Ibrahim R, et al. Instrumental vaginal delivery in Usmanu Danfodiyo University Teaching Hospital, Sokoto: a ten-year review. Trop J Obstet Gynaecol. 2018;35(2):168–72. https://doi.org/10.4103/TJOG.TJOG_13_18
- Alsheeha MA. Epidemiology of cesarean delivery in Qassim, Saudi Arabia. Open Access Maced J Med Sci. 2018;6(5):891–5. https://doi.org/10.3889/oamjms.2018.213
- Diaz V, Abalos E, Carroli G. Methods for the estimation of blood loss during childbirth. Cochrane Database Syst Rev. 2020;9:CD010980.
- Diaz V, Carroli G, Abalos E. Accuracy of visual estimation of blood loss in obstetrics: a systematic review. BJOG. 2021;128:969–77.
- Anger H, Durocher J, Dabash R, Winikoff B. How well do postpartum blood loss and common definitions of postpartum hemorrhage correlate with postpartum anemia and fall in hemoglobin?. PLoS One. 2019;14(8):221216. https://doi.org/10.1371/journal.pone.0221216
- Yefet E, Yossef A, Suleiman A, Hatokay A, Nachum Z. Hemoglobin drop following postpartum hemorrhage. Sci Rep. 2020;10(1):21546. https://doi.org/10.1038/s41598-020-77799-0
- Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika. 1965;52(3-4):591–611. https://doi.org/10.1093/biomet/52.3-4.591
- Hanley JA, Mcneil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143(1):29–36. https://doi.org/10.1148/radiology.143.1.7063747
- Mansukhani R, Shakur-Still H, Chaudhri R, Bello F, Muganyizi P, Kayani A, et al. Maternal anaemia and the risk of postpartum haemorrhage: a cohort analysis of data from the WOMAN-2 trial. Lancet Glob Health. 2023;11(8):e1249–1259.
- Mohammed A, Taye W, Tefera M, Ayele T. Immediate postpartum anemia and associated factors among women in public hospitals of Ethiopia: a cross-sectional study. Front Glob Womens Health. 2022;3:916245. https://doi.org/10.3389/fgwh.2022.916245
- Rakesh P, Gopichandran V, Jamkhandi D, Manjunath K, George K, Prasad J. Determinants of postpartum anemia among women from a rural population in southern India. Int J Womens Health. 2014 Apr;6:395-400. https://doi.org/10.2147/IJWH.S58355
- Atuahene M, Afari EO, Adjuik M, Obed S. Risk factors of anaemia among postpartum women in Bolgatanga Municipality, Ghana. BMC Res Notes. 2022;15:45.
- Abneh AA, Kassie TD, Gelaw SS. The magnitude and associated factors of immediate postpartum anemia among women who gave birth in Ethiopia: systematic review and meta-analysis. BMC Pregnancy Childbirth. 2024;24(1):317. https://doi.org/10.1186/s12884-024-06495-y
Keywords: Hemoglobin, Instumental vaginal delivery, estimated blood loss.

Publication History
Received: March 07, 2026
Revised: March 14, 2026 Revised: March 18, 2026
Accepted: March 25, 2026
Published: April 25, 2026
Authors
Maysoon Aladham
Department of Obstetrics and Gynecology, National Guard Hospital, Riyadh. Saudi Arabia.
Rana Ayed Alayed
College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh. Saudi Arabia.
Ghaida Mubarak Alotaibi
College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh. Saudi Arabia.
Deema Sameer Alzahrani
College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh. Saudi Arabia.
Fardus Salem Alsaiary
College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh. Saudi Arabia.
Hafiza Turkistany
Department of Obstetrics and Gynecology, National Guard Hospital, Riyadh. Saudi Arabia.